

Accountability
Dr Paul Alsop believes that accountability in skin cancer care requires transparency around outcomes, not just clinical intent.
To support this, histopathology results from skin cancer diagnosis and surgery are periodically reviewed and summarised as part of an outcomes audit.
The information below presents 2 audits of independently reported histopathology results across 5 clinics. In contrast to registry-based audits that rely on clinician self-reporting, this review is generated directly from pathology data, reducing reporting bias and providing an objective measure of outcomes.
Source: Pathlab and WBOP PHO credentialling audit 2026
For Patients
2026 Audit

How Dr Paul Alsop reviews the quality of his skin cancer work
Every lesion removed by Dr Paul Alsop is sent to an independent pathology laboratory (Pathlab) for analysis. These results are reviewed regularly to ensure important skin cancers are being identified and treated appropriately.
Independent audit results
Over a 12-month period:
813 skin lesions were reviewed using independent pathology data
47% were confirmed cancer or pre-cancer
33 melanomas were diagnosed
Melanoma detection
A separate independent audit examined lesions removed because melanoma was suspected.
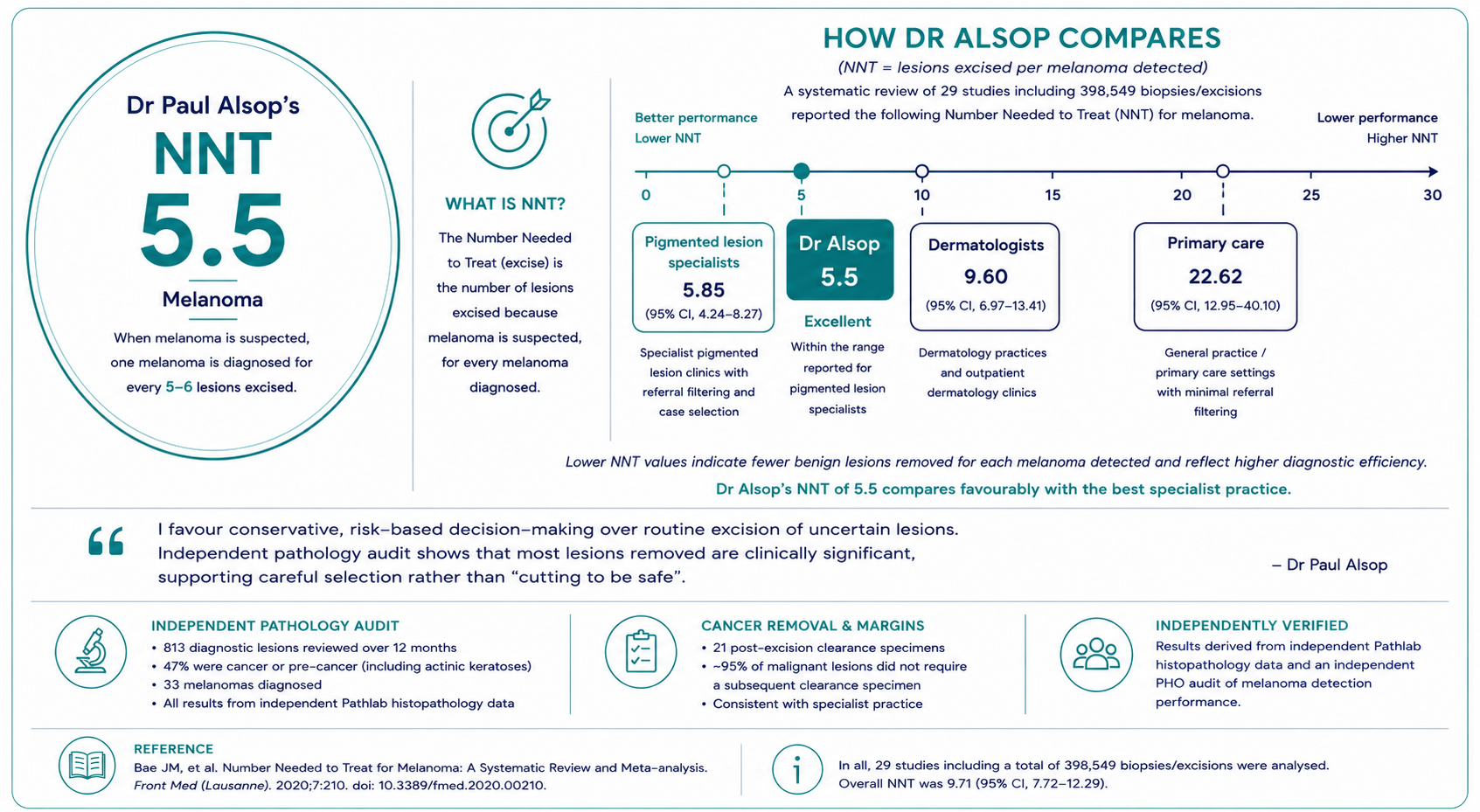
Melanoma NNT (Number Needed to Treat): 5.5
This means approximately one melanoma was diagnosed for every 5–6 lesions removed to exclude melanoma.
Published studies report melanoma NNT values ranging from approximately 4.7–22.6, depending on clinician experience and practice setting.
Cancer removal and margins
Twenty-one post-excision clearance specimens were recorded.
These represent planned follow-up procedures performed after a known cancer diagnosis, including wider excision after melanoma diagnosis and margin-control surgery where additional clearance was recommended.
Overall, approximately 95% of malignant lesions did not require a subsequent clearance specimen.
What this means for patients
These independent audits demonstrate a selective, risk-based approach to skin cancer care.
Rather than removing large numbers of harmless lesions "just to be safe", the aim is to identify clinically important skin cancers early while avoiding unnecessary procedures wherever possible.
The results show:
High rates of skin cancer detection
Melanoma detection performance that compares favourably with published studies
Most cancers managed without requiring further clearance surgery
Independent verification through pathology review rather than clinician self-reporting
Independent data sources
Results were derived from:
Independent Pathlab histopathology data covering all biopsied and excised lesions
An independent PHO audit assessing melanoma detection performance
Together, these provide an objective assessment of diagnostic accuracy and treatment outcomes.
For Clinicians

Independent histopathology audit — accession-level analysis
Data source: Pathlab histopathology export (.txt)
Audit unit: Unique pathology accession number (one specimen = one case)
Reporting basis: Independent laboratory data (not self-reported)
Dataset structure
Total accessions reviewed: 835
Diagnostic specimens included: 813
Post-excision clearance specimens: 21
Post-excision clearance specimens were analysed separately and excluded from diagnostic performance metrics.
Classification methodology
Lesion category assigned solely from the final Diagnosis field
Clinical indication, narrative, and microscopy text excluded
Each specimen assigned to a single diagnostic category
Actinic keratoses (AK) reported separately but excluded from primary benign-to-malignant (B:M) calculations
This approach prevents diagnostic inflation and ensures reproducibility.
Diagnostic yield and case mix
Among 813 diagnostic specimens:
384 malignant / pre-malignant lesions
429 benign lesions
This corresponds to:
47% malignant / pre-malignant
53% benign
The workload is therefore cancer-weighted and dominated by non-melanoma skin cancer.
Comparator context
General GP practice typically reports approximately 10–25% malignant lesions.
Mixed-interest skin practice commonly reports 25–35% malignant lesions.
GPwSI and dedicated primary care skin cancer clinics typically report 35–50% malignant lesions.
This audit demonstrated a malignant proportion of 47%.
Benign-to-malignant ratio (AK excluded)
Definitions
Malignant:
Basal cell carcinoma (BCC)
Squamous cell carcinoma (SCC, including SCC in situ)
Melanoma
Benign:
All remaining diagnoses
Excluded:
Actinic keratoses
Post-excision clearance specimens
Result
Benign-to-malignant ratio = 0.95 : 1
Comparator context
General GP practice commonly reports benign-to-malignant ratios of approximately 3–6 : 1.
Mixed-interest skin practice commonly reports 1.5–3 : 1.
GPwSI and dedicated primary care skin cancer clinics commonly report 1–2 : 1.
Published dermatology outpatient series typically report 0.6–1.5 : 1.
This audit therefore sits within the malignant-dominant end of specialist outpatient practice.
Melanoma detection performance
Whole-practice pathology audit
33 melanomas diagnosed
Approximately 25 diagnostic lesions per melanoma detected
This metric reflects overall pathology workload and includes non-melanoma skin cancers, actinic keratoses and benign lesions.
Melanoma-specific audit
An independent PHO audit reviewed lesions excised because melanoma was considered a possible diagnosis.
Melanoma NNT (Number Needed to Treat) = 5.5
This indicates that approximately one melanoma was diagnosed for every 5–6 lesions excised for melanoma exclusion.
Comparator context
A systematic review and meta-analysis of melanoma Number Needed to Treat (NNT) reported the following ranges:
General practitioners: NNT approximately 9.6–22.6
Dermatologists: NNT approximately 4.7–9.6
Pigmented lesion clinics and specialist melanoma services: often <5–10, depending on referral filtering and case selection
Post-excision clearance and margin management
Twenty-one post-excision clearance specimens were identified.
These specimens represent planned margin assessment following a known diagnosis of skin cancer and may include:
Wider excision following melanoma diagnosis
Margin-control procedures
Management of incompletely excised tumours
Additional clearance where recommended by pathology
They do not represent new diagnostic decisions and were therefore excluded from diagnostic yield calculations and benign-to-malignant ratios.
Overall, approximately 95% of malignant lesions did not require a subsequent clearance specimen.
Comparator context
Published incomplete excision or planned re-excision rates are approximately:
General practice: 8–30%
GPwSI skin cancer practice: 2–5%
Dermatology and plastic surgery series: 2–5%
Observed clearance rates in this audit are consistent with specialist practice.
Methodological strengths
Accession-based analysis
Independent pathology source
Explicit inclusion and exclusion criteria
Separation of diagnostic and post-treatment specimens
Reproducible methodology derived from raw Pathlab exports
Independent PHO verification of melanoma detection performance
Summary
This audit demonstrates a cancer-weighted case mix, malignant-dominant benign-to-malignant ratios, efficient melanoma detection, and structured margin management.
Results are derived from independent pathology data and supported by a separate melanoma-specific PHO audit, providing transparent and reproducible measures of diagnostic performance and treatment outcomes.
“Pathology audit findings are consistent with a high-threshold, oncology-focused approach to lesion management, prioritising diagnostic yield and surgical quality over volume.”
Comparator data are included for contextual reference only and should not be interpreted as formal benchmarks, thresholds, or indicators of clinical performance.
Data analysis was performed with the use of raw data processed manually in MS Excel, then verified with reproduciable AI data prompts:
“Analyse a raw Pathlab histopathology export (.txt) using specimen-level analysis.
Use the laboratory accession number as the unique unit of analysis (one specimen = one case).
Classify lesions strictly from the final Diagnosis field only; ignore narrative history, microscopy text, and clinical indication fields.
Group diagnoses into: basal cell carcinoma (BCC), squamous cell carcinoma (including SCC in situ), melanoma (in situ and invasive), actinic keratosis (AK), benign melanocytic lesions, other benign lesions, and post-excision clearance specimens.
Exclude AK-only specimens from primary benign-to-malignant ratio calculations.
Count post-excision clearance specimens separately and exclude them from diagnostic yield metrics.
Calculate absolute counts, benign-to-malignant ratios (with and without AK), percentage malignant, lesions-per-melanoma ratio, and first-pass complete excision rate based on margin status where applicable.
Do not infer diagnoses from partial text or assumptions.
Return results as reproducible summary metrics consistent with independent pathology audit methodology.”
References
SCARD Systems.
Report for the SCARD Research Pool.
Reporting period: 1 Feb 2025 – 16 Feb 2026.
(287 clinicians; 121,929 lesions)Murchie P, et al.
Diagnostic accuracy of skin cancer excisions in primary care: a retrospective observational study.
British Journal of General Practice. 2011;61:e563–e569.Goulding JMR, et al.
The accuracy of skin cancer excision by general practitioners in primary care.
British Journal of Dermatology. 2001;145:884–888.Reid CM, et al.
Skin cancer management by general practitioners with advanced training.
Medical Journal of Australia. 2010;193(6):328–332.Roozeboom MH, et al.
Incomplete excision of basal cell carcinoma: a systematic review.
British Journal of Dermatology. 2012;167:353–361.Bath-Hextall FJ, et al.
Surgical excision versus other treatments for basal cell carcinoma.
British Journal of Dermatology. 2007;156:848–857.Rowe DE, Carroll RJ, Day CL.
Long-term recurrence rates in previously untreated basal cell carcinoma.
Journal of the American Academy of Dermatology. 1989;21(5):756–764.Leffell DJ, et al.
Surgical treatment of nonmelanoma skin cancer.
New England Journal of Medicine. 2001;345:976–983.Hallock A, et al.
Audit of skin lesion excision and diagnostic yield in primary care.
British Journal of Dermatology.English DR, et al.
Incidence of cutaneous melanoma and diagnostic accuracy in primary care.
Medical Journal of Australia.Australian Skin Cancer Audit Research Database (SCARD).
SCARD Research Pool Outcomes Report.Australian Skin Cancer Audit Research Database (SCARD).
SCARD Methods and Definitions Document.